Introduction and Definitions
Pelvic congestion syndrome (PCS) is a source of chronic pelvic pain in women caused by venous obstruction and retrograde flow in an ovarian vein.
PCS is considered the female equivalent of scrotal varicocele.
PCS is often misdiagnosed,
or clinicians fail to consider it in the large differential diagnosis of chronic pelvic pain.
In addition,
patients may fail to alert their healthcare provider to symptoms of mild chronic pelvic pain in the mistaken belief it is due to dysmenorrhea.
Etiology and Pathophysiology:
PCS can occur in a primary form caused by incompetent valves in the ovarian and internal iliac veins or in a secondary form due to obstructed or compressed veins.
Incompetent ovarian vein valves lead to venous reflux and retrograde flow.
Both forms of PCS,
primary and secondary,
cause blood flow to be diverted to the pelvic veins,
which in turn leads to congestion and engorgement of pelvic veins (i.e.,
varices or varicosities) and ultimately to chronic pelvic pain.
The most common causes of secondary PCS are:
- Compression of the left common iliac vein by the crossing right common iliac artery (May-Thurner Syndrome)
- Compression of the left renal vein between the superior mesenteric artery and abdominal aorta (nutcracker phenomenon)
- Retroaortic left renal vein
Primary PCS:
It is estimated that 10% of women have incompetent ovarian vein valves.
Approximately 40-60% of these women reported chronic pelvic pain compatible with PCS.
Among the symptomatic women,
75% saw improvement after ovarian vein ligation.
However,
the clinical significance of ovarian vein reflux in asymptomatic women is unclear and controversial.
Among women undergoing conventional angiography for reasons other than suspected PCS,
approximately 10% showed retrograde ovarian vein flow.
Treatment options for primary PCS include ovarian vein ligation or embolization to prevent ovarian vein reflux.
Both options have shown high success rates and are currently the first-line therapies.
Reliably identifying ovarian vein reflux in symptomatic patients is considered the key to imaging diagnosis and is probably the most important determinant of therapeutic response to ovarian vein ligation or embolization.
Fig. 1: Coronal MIP cine loop from contrast-enhanced time-resolved 3D MRA shows early retrograde filling of a markedly dilated left ovarian vein in a different patient with subsequent filling of periuterine varices.
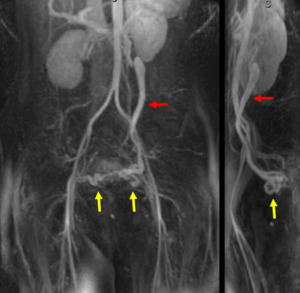
Fig. 2: Coronal (left) and sagittal (right) MIP images from a contrast-enhanced time-resolved 3D MRA MIP show early retrograde filling of a dilated left gonadal vein (red arrow), and right and left periuterine varices in the pelvis (yellow arrows).
Nutcracker syndrome
Nutcracker syndrome,
also known as left renal vein entrapment syndrome,
is observed when the superior mesenteric artery (SMA) makes an abnormally acute angle with the aorta (< 60°) and extrinsically compresses the left renal vein between the SMA and abdominal aorta.
Consequently,
venous return from the left kidney is forced to find a lower resistance pathway to the IVC,
such as an incompetent left ovarian vein.
Several studies have reported that 20-30% of patients with PCS had nutcracker syndrome.
This subset of PCS patients can also present with flank pain and hematuria due to renal venous hypertension.
A knowledge of the anatomic pathology of nutcracker syndrome is important in guiding surgical or endovascular interventions to alleviate PCS symptoms.
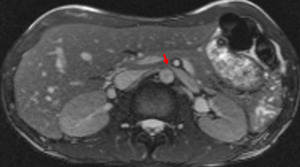
Fig. 3: Axial balanced SSFP image showing the compression of the left renal vein
Imaging features:
Conventional angiography:
Conventional angiography,
including pelvic and ovarian vein venography,
was considered the traditional gold standard for evaluating PCS.
However,
conventional angiography has several drawbacks -- it is invasive,
time-consuming,
uses ionizing radiation,
and requires iodinated contrast.
Also,
antegrade or retrograde injection of contrast material into the ovarian veins may alter the normal venous hemodynamics,
thereby decreasing the specificity and specificity of conventional angiography.
CT,
MRI and Ultrasound:
Noninvasive imaging techniques used for the workup of suspected PCS include CT and static MRI (i.e.,
without time-resolved imaging).
In studies using CT or static MRI to investigate the prevalence of ovarian vein reflux in asymptomatic women,
the reported prevalence was 35-50% based on ovarian vein diameter and contrast characteristics.
However these studies lacked correlation with conventional venography as the gold standard.
Contrast-enhanced MRA (CE-MRA) performed reasonably well for detection of ovarian vein reflux,
showing a high sensitivity of 88%,
but a lower specificity of 67%.
A weakness of CT and static MRI for diagnosing PCS is that they rely on indirect findings to identify incompetent valves and retrograde flow in the ovarian veins.
Indirect findings include pelvic varicosities and a dilated ovarian vein that opacifies early.
However,
these findings are nonspecific.
For example,
pelvic veins can become dilated for a variety of reasons,
such as prolonged standing or portal hypertension.
More importantly,
CT and static MRI fail to unequivocally determine if ovarian vein flow is antegrade or retrograde - a key to diagnosing PCS.
Another issue concerns the patient position in the CT or MRI scanner.
Abnormal ovarian veins with incompetent valves may appear nondilated when the patient is supine.
Transvaginal ultrasound (TVUS) is often the first-line imaging modality for evaluating women with chronic pelvic pain.
When combined with Doppler,
TVUS can identify many key imaging findings of PCS,
such as ovarian vein dilatation,
retrograde flow,
and pelvic varicosities.
TVUS can also help to exclude alternative diagnoses for pelvic pain.
Weaknesses of TVUS include operator dependence and a limited ability to demonstrate vascular continuity over a large anatomic region.
Time-resolved MR angiography (TR-MRA):
Time-resolved MR angiography (TR-MRA) offers a rapid and noninvasive method for visualizing vascular anatomy and blood flow dynamics.
Several studies have shown that TR-MRA has high sensitivity and specificity,
comparable to conventional angiography,
for detecting anatomic and hemodynamic pathology in a variety of vascular beds.
One technical challenge of TR-MRA is to determine the optimal tradeoff between temporal and spatial resolution to answer the specific clinical question.

Fig. 4: Coronal MIP cine loop from contrast-enhanced time-resolved 3D MRA shows early retrograde filling of a mildy dilated left ovarian vein with subsequent filling of periuterine varices.

Fig. 5: Coronal MIP image obtained during the arterial phase of a contrast-enhanced time-resolved 3D MRA in a different patient shows early reflux of contrast into a dilated left ovarian vein (red arrow).
In patients with suspected PCS,
TR-MRA provides dynamic imaging of the lower abdominal and pelvic veins and the ability to detect retrograde flow in the ovarian vein,
a finding which is critical to establishing the diagnosis.
In fact,
several studies have shown that TR-MRA reliably depicts the venous abnormalities of PCS.
Findings of primary PCS on TR-MRA include early retrograde opacification of a dilated ovarian vein,
followed sequentially by early opacification of ipsilateral periuterine varices,
cross-filling of contralateral periuterine varices,
and normal antegrade opacification of the contralateral ovarian vein.
A study by Kim et al.
showed significant variability in the time to visualize ovarian vein reflux after aortic opacification with an average of 15 seconds (range of 7–32 seconds).
This variability underscores the importance of using a time-resolved imaging technique with a long acquisition window.
TR-MRA can also identify ovarian vein reflux caused by nutcracker syndrome.
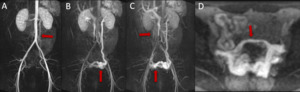
Fig. 6: Sequential MIPs from contrast-enhanced time-resolved 3D MRA showing early retrograde opacification of a dilated left ovarian vein ( arrow) at 6 seconds (A), filling of the left periuterine varices (arrow) at 12 seconds (B), cross-filling of right periuterine varices at 42 seconds (arrow), and normal antegrade filling of a non-dilated right ovarian vein(arrow) (C). Axial MIP (D) from contrast-enhanced time-resolved 3D MRA shows cross-filling of periuterine varices from left to right via a dilated arcuate vein in the uterine myometrium.
TR-MRA of the renal,
ovarian and pelvic veins requires the injection of only a small volume of gadolinium-based contrast via a peripheral IV,
thereby limiting any potential interference with venous hemodynamics.
By comparison,
conventional angiography of the left ovarian vein requires a substantial contrast volume and a high injection rate in order to overcome high renal vein blood flow.
Thus,
conventional angiography has the potential to alter normal venous hemodynamics and cause retrograde flow into a left ovarian vein with competent valves.
Consequently,
TR-MRA may provide a more accurate depiction of the physiologic hemodynamics of the left ovarian and pelvic veins.
TR-MRA could become the gold standard for evaluating women with chronic pelvic pain and suspected PCS.
Moreover,
the combination of TR-MRA and standard pelvic MRI can be used to identify alternative causes of chronic pelvic pain.
Fig. 7: Cine clip of rotating MIP images from the late arterial phase of a contrast-enhanced time-resolved 3D MRA shows dilated left ovarian vein and periuterine varices. It is possible to generate the rotating MIP images because the raw data at each time frame is volumetric (3D).
Valsalva maneuver
The Valsalva maneuver and table tilting have been advocated to increase the conspicuity of dilated and incompetent ovarian veins by promoting retrograde flow and venous engorgement during conventional angiography,
CT and ultrasound.
With TR-MRA,
retrograde flow in a non-dilated ovarian vein with incompetent valves can ordinarily be visualized,
but adding the Valsalva maneuver may improve sensitivity,
especially when the reflux is very slow.
However,
an exceptionally forceful Valsalva maneuver may -- at least theoretically -- cause reflux into an otherwise competent ovarian vein.


 and sagittal (right) MIP images from a contrast-enhanced time-resolved 3D MRA MIP show early retrograde filling of a dilated left gonadal vein (red arrow), and right and left periuterine varices in the pelvis (yellow arrows).")


.")
 at 6 seconds (A), filling of the left periuterine varices (arrow) at 12 seconds (B), cross-filling of right periuterine varices at 42 seconds (arrow), and normal antegrade filling of a non-dilated right ovarian vein(arrow) (C). Axial MIP (D) from contrast-enhanced time-resolved 3D MRA shows cross-filling of periuterine varices from left to right via a dilated arcuate vein in the uterine myometrium.")
.")